
Parents often ask – “what is the best nipple to use for bottle-feeding my baby?” For most healthy, full-term babies, it really might not matter. Most of these babies will be able to manage the flow from any bottle nipple intended for newborns. Healthy, full-term babies are able to reduce sucking pressure or alter their sucking rate to manage milk flow. These babies also tend to have relatively good overall tone and are able to effectively swallow and protect their airway from fluid penetration. On the other hand, for babies who are born preterm (even late preterm at 34-37 weeks) or with other conditions that contribute to feeding difficulty (e.g., congenital heart disease, low tone), FLOW MATTERS!
Why does flow matter?
When a baby is exposed to milk flow from a bottle, he has four options: swallow, drool, pool or refuse all together. Every time a baby swallows, their airway is closed for about a second. The higher the flow, the more they are going to be required to swallow in order to keep from drooling or pooling. Alternatively, as milk flow is slowed, it takes longer to accumulate a bolus, swallowing rate is reduced, and the infant has more time to breathe during feeding. For the infant with respiratory or cardiac disease, this difference in flow may the difference that allows them to maintain oxygenation throughout feeding and keep from becoming fatigued to the point that they are no longer able to continue. For the baby with low tone or with swallowing difficulty, slowing the flow allows them a longer period of time to coordinate a safe swallow and to completely clear the oropharynx of fluid before another bolus accumulates, reducing the likelihood of aspiration.
When flow is fast, the infant with feeding difficulty often creates a loose latch in order to slow the flow. From the feeder’s perspective, the nipple is easily pulled from the baby’s mouth or it sometimes looks like the baby is chewing on the nipple. This is an effective strategy to keep from becoming overwhelmed by fluid, but it is usually not an effective feeding strategy for transferring the nutritional content needed for adequate growth. It also does not “exercise” the musculature that is required for long-term bottle and breast-feeding, and for later oral feeding and language skills.
Nipples are labeled with names such as slow, standard, preemie, level 1, newborn flow – what does it all mean? Parents and clinicians are often overwhelmed with options for bottle-feeding infants, but there really is very little information to help guide decision-making, especially for medically fragile infants who need to be supported during their learning to orally feed.

Nipple Flow Rate Study
We tested the nipples most frequently used for feeding infants in the hospital and in the community. We developed a standardized testing procedure using a breast pump to simulate sucking and measured the amount of formula expressed in one minute. 45 different types of nipples were tested. For each nipple type, 10 nipples were tested to give us information about the average flow rate and variability. The milk flow rates described are not necessarily the rates that an infant will achieve when feeding. Infants feed with varying sucking pressures and rates, so they will achieve varying flow rates even from the same nipple. The results of this study should be interpreted as a means of comparing nipples to one another. For more information about our methods, please feel free to contact me.
Testing Set-up

Results
Milk Flow Rates
(double click on graph to enlarge)

Pados Graph 1 for Blog Post PDF-2 copy
What we found was very interesting. There was a wide range of flow rates from the nipples tested, from less than 2 mL/min to more than 80 mL/min. The name of a nipple does not always give an accurate indication of how fast or slow it may actually be. Among the nipples used for feeding hospitalized infants, we were interested to find that for both the Enfamil and Similac brands, their single-use premature nipples were faster than either their slow or standard flow nipples. This is not entirely surprising as many clinicians have suspected that the Similac Premature (red nipple) was a very fast nipple. Interestingly, the Enfamil Slow nipple was found to be quite fast, even faster than the Similac Premature. The Avent Natural Newborn was the slowest nipple we tested, followed by the Enfamil Cross-cut, new Dr. Brown’s Ultra-Preemie nipple, and Bionix level 1. Please note that Dr. Brown’s Y-cut nipple was tested with standard-thickness formula. In practice, this is often used with thickened milk. Also, the results of the cross-cut should be interpreted with caution since only negative pressure was applied during our testing. The application of positive pressure during feeding changes the shape of the cross-cut and likely changes the flow rate.
Variability
(double click on graph to enlarge)
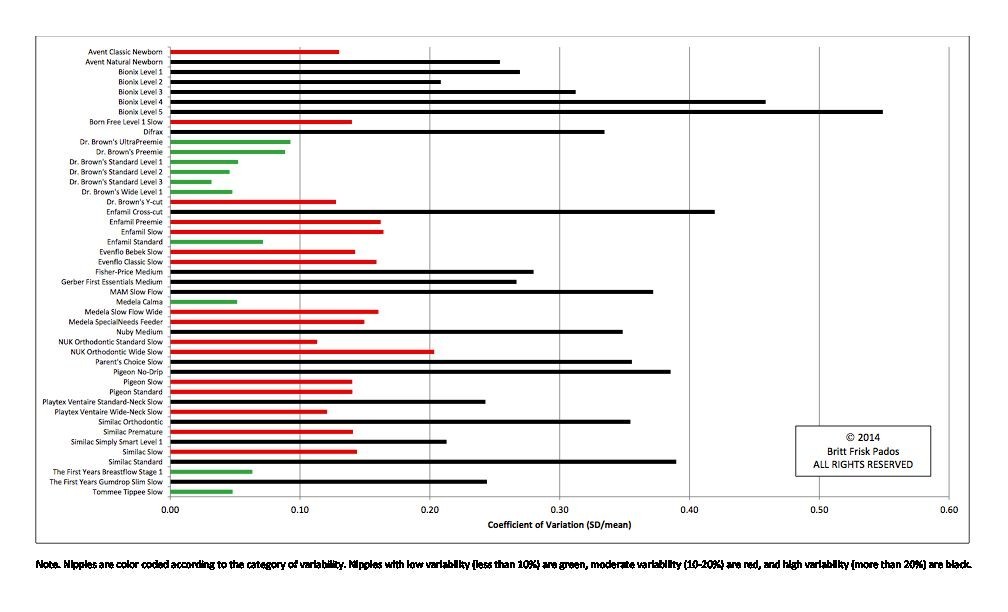
Pados Graph 2 for Blog Post PDF copy
There is also a lot of variability in the flow rates of certain nipples. This means one nipple to the next of the same type varies in flow rate. Only 10 of the 45 nipples tested were found to have low variability (less than 10% variation between nipples). The Dr. Brown’s brand was the most consistent brand with 6 of their nipples having low variability. Tommee Tippee, The First Years Breastflow, Medela Calma, and Enfamil Standard were the other nipples with low variability. 19 of the nipples tested were found to have high variability (more than 20% variation).
The idea of variability among nipples is important. As medically fragile infants are learning to eat, we often find that there is significant variability in how they feed from one feeding to another. We often assume that this is variability within the infant (i.e, level of fatigue), but some of that variability may actually come from the nipple as well. We need to keep this in mind. For example, if an infant is not feeding well, this study shows that it may be worth trying a different nipple of the same type or it may be worth changing to a nipple which has been shown to have less variability than others.
Other interesting findings:
-
Some of the nipple holes were not open.
-
As formula was exposed to air for a period of time, it thickened and slowed flow rate. We periodically changed the formula to prevent this from affecting our results.
-
Tightening the nipple to the bottle too much can prevent the equilibration of pressure within the bottle. This results in a build-up of suction pressure in the bottle and can cause the nipple to collapse. In practice, this would make it harder and harder for an infant to suck fluid from the nipple. We tightened the nipple to the bottle until it felt tight and then loosened about a ¼ of a turn.
-
The more fluid there is in the bottle, the more gravitational pressure will be placed on the nipple, increasing flow. Alternatively, less fluid in the bottle will decrease flow rate. We made sure we adjusted for this in our tests.
Take away points
-
There is a wide variety of flow rates of nipples available for feeding infants.
-
Infants at risk for or who have feeding difficulty should start with the slowest flow nipple available.
-
For very vulnerable babies who are being fed from ready-to-feed formula bottles, consider discarding any unneeded formula prior to feeding to reduce flow rate.
-
If an infant is having unusual difficulty with a particular feeding, it may be worth changing to a different nipple of the same type (especially if it is one that was found to be highly variable) or change to a nipple that was found to be less variable.
-
If an infant appears to be sucking well, but is not transferring milk, check to make sure the nipple hole is open and reapply the nipple to release suction.
-
When an infant is ready for discharge from the hospital, consider choosing a nipple of comparable flow to that used successfully in the hospital. Having parents bring the nipples that will be used at home into the hospital prior to discharge is helpful to make sure the infant can feed safely before discharge.
Britt Pados is a Neonatal Nurse Practitioner and a doctoral candidate in the School of Nursing at University of North Carolina at Chapel Hill. She can be contacted at bpados@email.unc.edu. This study was conducted by researchers from the Feeding Flock Feeding Interest Group at the University of North Carolina, including Britt Pados, PhD(c), RN, NNP-BC, Jinhee Park, PhD, RN, Suzanne Thoyre, PhD, RN, FAAN, Hayley Estrem, PhD(c), RN, and Brant Nix, BMET, BA.

The Feeding Flock Feeding Interest Group at the University of North Carolina Chapel Hill is a multidisciplinary group of researchers and clinicians interested in helping families nurture children with feeding difficulties. We are in the process of developing several questionnaires to measure problematic feeding behaviors, skills related to feeding, and family management of feeding difficulty in children. We are currently seeking families who have children with feeding difficulty and are interested in helping us with our research to join the Feeding Challenges Registry. For more information please visit our website at: http://feedingflock.web.unc.edu/
What fantastic information-everytime I read your blog, I feel like I’m getting a days worth of information that I would get from a course. Thank you for sharing your knowledge on this blog! My colleague and I weren’t sure how we came to know about it, but my goodness, we frequently discuss the things we read on here and how we can apply the principles in our clinic. Thank you thank you thank you!
Thank you! Krisi
We have a 3 month/ 6 weeks adjusted age infant at home. We’ve been using the Dr. Brown’s Preemie nipples since we left the hospital and he does well, but feeding towards the end takes a LONG time. Overall he takes about 30-40 minutes depending on sleepiness.
When we first brought him home, he was a VERY messy bottle eater. He’s improved significantly in the last 4 weeks and is steadily gaining weight, but I wonder if and when we should switch to another nipple.
Would say the Dr. Brown’s Ultra Preemie strengthen his sucking mechanism? Would a level 1 allow him to feed more efficiently?
Any help would be appreciated.
Sounds like he should’ve been started on an Ultra to develop coordination prior to discharge. They are sometimes unpopular with certain hospitals/nursing staff. Viscosity of liquids have to be taken into account. Breast milk (even fortified 26 cal) falls within “very thin” viscosity rating on the new rating system. Formulas are considerably thicker, and could be a little more difficult to extract from an ultra. What you need to look at is Why baby is taking more than 20-25 mins to feed… are they sucking vigorously? Are they breathing heavily or loudly during breathing beaks? ? How is weight gain? The gold standard is 1-2sucks;swallow;breathe per second if baby is swallowing more than once per swallow, flow rate is possibly too high. If baby was a messy eater going home, I would ask your pediatrician about available outpatient speech therapy clinics that could do an assessment and help you get to a better bottle system for your baby. If a level 1 is too fast in Dr. B and baby is inefficient with preemie, sometimes you can use a Dr. B infant paced valve to increase efficiency. Be aware that the valve will maximize bolus extraction for that flow rate, so recommend going down one flow rate in nipple if baby already showing signs of inefficient extraction. A Speech Language Pathologist who specializes in pediatric feeding can help you get a system that will work for you.
My 7 week old is on similac for spit up it seems to be thicker than his last formula. He was not getting any of the new formula with his old nipples it was like it was not coming through . We used slow flow Dr browns and mam infant but have switched to dr browns size 2 medium flow nipple, he’s doing fine with it what is your thoughts, is it to soon for medium flow?
Thank you this was very useful
Did you consider that the flow rate is dependent on the negative pressure building up inside the bottle? As you say, if such pressure builds up inside the bottle that baby has to such harder because the flow rate slows down…
Than you for sharing.
My baby is 6 months ,we been useing a preemie nipple thought it was time to up up but she still makes a mess milk just flows out her mouth what she I do we waste a lot of milk
This is a very helpful study, so thank you! The only information I wish was also tested and included would be regarding pumped breast milk. I’d like to know how breastfed babies respond to different types of slow flow nipples (because it is common for breastfed babies to start to prefer the faster flowing bottles over nursing).
Can you tell me which nipple over all has the lowest flow. I an a Wildlife Rehabber and I have 2 raccoons approximately 2.5 weeks old. Every nipple I’ve tried is allowing them to aspirate the formula
I have a 8 month old. Every time I use medium flow it seems like she chokes because its going too fast, but when I use slow flow its too slow. What should I do?? She uses similac sensitive, and she still is spitting up after every feed.