
 Written by Kerry Gibson RD, CNSC, LDN, UNC Pediatric Feeding Team Dietician
Written by Kerry Gibson RD, CNSC, LDN, UNC Pediatric Feeding Team Dietician
From the UNC Feeding Team Blog, https://uncfeedingteam.web.unc.edu
Children with feeding disorders may require G-tube feeding to assist them in meeting their nutrient requirements. G-tube feedings may be given with a commercial formula, homemade blenderized tube feeding or commercialized blenderized tube feeding. The medical team (physician, nurse practitioner, registered dietitian and feeding therapist) can help to guide decision making on which formula is best for each child.
Parents who choose blenderized tube feeding often do so due intolerance of commercial feeding formula, food allergies, desire to use “real food” or for improvement in GI symptoms such as gagging, retching, vomiting, reflux and constipation. When choosing to use blenderized tube feeding you have the option of using a commercial blenderized tube feeding or homemade blenderized tube feeding.
Homemade blenderized tube feedings are less expensive and can give more of a variety of foods. However, they also can raise food safety concerns, have a short hang time (~2 hours), may have unpredictable nutrient levels by using non-standardized recipes and are not often covered by insurance. Choosing homemade blenderized tube feeding will require close work with a registered dietitian to ensure adequate nutrients are provided.
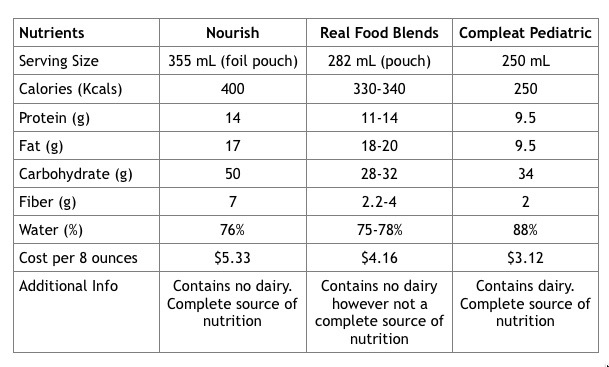
Commercial blenderized tube feedings are convenient, processed to ensure food safety, have a longer hang time of 8-12 hours, standardized nutrient levels and may be covered by insurance. Below is a comparison of several commercial blenderized tube feedings:

{kind=link}
What micronutrients are missing from Real Food Blends that causes you to categorize it as “not a complete source of nutrition”? The macronutrients and calories are roughly comparable to Nourish and Compleat Pediatric.
To answer the questions posed, we agree that every child who eats by mouth does not have their meals evaluated for nutrients and micronutrients. Most RD’s will recommend that children and adults take a daily MVI even if you eat a variety of foods as it is very difficult to consume all required nutrients on a daily basis.
With that said children that require TF are usually medically complex, they can be underweight or malnourished therefore in order to optimize their growth and development we need to pay closer attention to what they are receiving on a daily basis with their TF formula.
When I wrote this post I gathered information directly from the manufacturer. Real Food Blends website in the FAQs section states that their product was not designed to be sole source of nutrition. The manufacture themselves are stating that their product is deficient in some micronutrients and that if a patient chooses to use it as a sole source of nutrition then they will have to discuss this with a dietitian and “take an age appropriate MVI and a dash of salt”. Please see the manufactures explanation below.
The same way that oral eaters need to eat a wide variety of foods over the course of a day or week to achieve necessary nutrient goals, our meals are just that – meals. They are each well-balanced and together offer a good variety. We developed these first meals with the intention that someone who is living off 6 or 8 cans of formula a day could easily add some nutritional variety to their diet with the addition of our meals. Those that already blenderize for tube-feeding can use our meals as a convenient option.
If you are using our meals as a sole source of nutrition (so getting nothing else), you will need to take an age-appropriate multivitamin and a dash of salt daily. Please discuss with your dietitian. If you take a look at the ingredients list in a can of regular formula. Most of the ingredients are added vitamins to make them nutritionally complete – something you can easily do with a multi-vitamin.
Aside from nutritional variety, we hope that giving a few different meals to tube-fed people will have a positive psychological impact. These are meals similar to what the rest of the family is getting. (The last thing someone with a tube wants is to be further isolated or different!) Also, many tube-fed adults report that they can still experience some taste sensation through burping and smelling their food. Part of the reason some report disliking formula so much is regurgitation or smelling the same thing over and over again. This is why we have added a spice to some of our meals and hope that our customers enjoy the variety.
You can also find the nutritional data sheets of each formula on their website. To specifically answer the question of what micronutrients are missing from each formula I have summarized below:
Beef, Potatoes and Peas formula is lacking Vitamin E and Iodine
Orange Chicken, Carrots and Brown Rice formula is lacking Vitamin E, Vitamin D, Biotine and Chloride
Salmon, Oats and Squash formula is lacking Vitamin E, Vitamin D, Iodine, Biotin, Chloride, Chromium and Molybdenum
Quinoa, Kale and Hemp formula is lacking Vitamin E, Iodine, Biotin, Choline, Chloride, Chromium and Molybdenum
The blog post was not written with the intent to sway parents to choose one formula over the other, it was written to show the options available to parents with facts provided from the manufactures so the parents and their medical team can make an educated decision on which formula could best meet the nutrient needs of their child.
Kerry Gibson RD,LDN,CNSC| Outpatient Pediatric Dietitian
UNC Hospitals
101 Manning Drive, Chapel Hill, NC 27514
(984) 974-9500
kerry.gibson@unchealth.unc.edu